Vocal nodules typically occur as a result of voice misuse or voice overuse. They are sometimes called “singer’s nodules” or “screamer’s nodules” (perhaps depending on the quality of the individual’s voice!!). They most often are bilateral and occur at the junction of the anterior one-third and the posterior two-thirds of the vocal folds. This is the mid-portion of the membranous vocal folds (the posterior portion of the vocal fold is made of more rigid cartilage), and it is generally felt that this part of the vocal fold receives the most contact injury during speech.
The actual injury that occurs there represents a continuum of changes. Initially, the vocal folds become swollen (the medical term for swelling is “edema”). With continued misuse, the edema increases and the nodules enlarge and harden. Over time they can become quite hard and fibrotic, similar to a callous.
The nodules are located in the very superficial layer of the vocal fold. They interfere with the mucosal wave and can cause hoarseness. Occasionally only a certain pitch range will be affected.
Treatment of vocal fold nodules is initially voice therapy. The goal is to minimize those types of voice use that traumatize the folds. In most cases the nodules will respond well to therapy alone (especially if they are diagnosed at an early stage. If the nodules persist despite therapy, they may need to be removed surgically. This is done through the mouth using a microscope under high magnification and special microlaryngeal instruments.
The picture to the top-left shows typical vocal fold nodules. (Anterior is to the top, and posterior is the back. Note that they are present on both vocal folds and in this case are actually quite symmetric. The are located about one-third of the way back on the vocal folds.
Vocal Fold Cysts
Vocal fold cysts are benign lesions as well. but unlike nodules they often are not associated with voice misuse or voice overuse. A cyst is simply a fluid collection in a sac-like structure. The vocal folds are lined with many small glands that secrete mucous. This mucous helps the folds vibrate more easily. Occasionally one of these glands will not drain properly and fluid will accumulate. This accumulation of mucous produces vocal fold cysts.
Vocal fold cysts differ from nodules in that they often occur only on one fold and are not in the same classic location as vocal fold nodules. They also seldom respond to voice therapy and therefore more frequently need to be surgically removed. The surgery is done with microlaryngeal instruments, with the goal of preserving the normal structure and function of the vocal fold as much as possible. In particular, the thin covering of the vocal fold should be preserved and there should be as little scarring as possible.
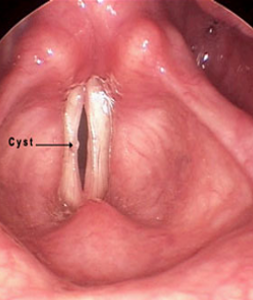
The image to the right shows a vocal fold cysts in a soprano who had significant hoarseness. This picture was taken with a stroboscopic light source through a flexible fiberoptic scope. The vocal folds are therefore “frozen” in time at the point of closure. Note that the folds cannot close completely due to the cyst. This cyst was removed surgically and the voice returned to normal.
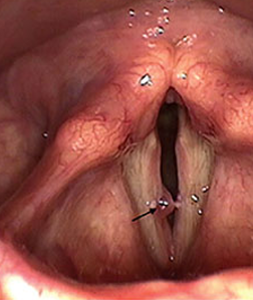
This image shows a close up view of a larger cyst in a different individual. This photograph was taken at the time of surgery for removal of the cyst. Notice that the left vocal fold is slightly thickened immediately opposite the cyst. This thickening has developed in response to the cyst, and should resolve spontaneously after removal of the cyst.
The to the the right shows bilateral cysts on vocal folds that may have developed at the site of previous nodules. The cyst on the right is more solid in appearance but did contain fluid. The cyst on the left has a little dark red dot showing where there has been bleeding into the cyst.
Vocal Fold Nodules
The image to the right shows a vocal fold cysts in a soprano who had significant hoarseness. This picture was taken with a stroboscopic light source through a flexible fiberoptic scope. The vocal folds are therefore “frozen” in time at the point of closure. Note that the folds cannot close completely due to the cyst. This cyst was removed surgically and the voice returned to normal.
This image shows a close up view of a larger cyst in a different individual. This photograph was taken at the time of surgery for removal of the cyst. Notice that the left vocal fold is slightly thickened immediately opposite the cyst. This thickening has developed in response to the cyst, and should resolve spontaneously after removal of the cyst.
The to the the right shows bilateral cysts on vocal folds that may have developed at the site of previous nodules. The cyst on the right is more solid in appearance but did contain fluid. The cyst on the left has a little dark red dot showing where there has been bleeding into the cyst.
Purpose of review:
Since the introduction of endolaryngeal microsurgery, several basic microsurgical techniques have been described for the removal of benign vocal fold lesions. These techniques include conventional incision or dissection, bimanual retraction and cutting, microflap technique and the CO2 laser. Until recently, only a few microsurgical methods have emerged as new choices for the treatment of benign vocal fold lesions. This article introduces an innovative method that can precisely remove benign sessile vocal fold lesions with epithelial keratosis or hyperplasia without jeopardizing the intermediate or deep layer of the lamina propria.
Recent findings:
Instead of using conventional vertically opening microinstruments, this microsurgical pressing excision technique (MPET) utilized two pairs of custom-made horizontally left-opening or right-opening, curved microscissors/curved cupped microforceps to remove right or left vocal fold lesions accordingly. Using one instrument at a time, the lesion was subsequently removed with the microscissors and microforceps in a press-evert-cut manner. Among a total of 553 cases, the treatment results were satisfactory, with 520 (94%) patients retaining a satisfactory/normal (G0) voice 2 months postoperatively. More importantly, no patient’s voice was worse postoperatively.
Summary:
This technique has several advantages: utilizing one instrument at a time can maximize exposure of the narrow endoscopic view, adjusting the pressing force makes precise excision easy in a well controlled horizontal plane. The MPET is particularly useful for removing sessile vocal nodules (especially those with epithelial keratosis), epithelial hyperplasia and leukoplakia in patients with difficult endolaryngeal exposure. This could be a well tolerated and precise microsurgical technique.
While the effectiveness of autogenous fat augmentation after microsurgical removal (FAMSR) of the vocal nodules (VN) has been previously shown in patient treatment programs, relatively little information is available regarding the long-term effectiveness of such a procedure. This paper examines, in retrospect, the long-term effectiveness of FAMSR in patients with VN (n = 41) using pre- and post-FAMSR perceptual acoustic and phonatory function data and videolaryngostroboscopic findings for 33 patients. The mean follow-up time was 18 months. Thirty-three (80.4%) patients displayed excellent results; 4 (9.8%) experienced improvement, and 4 (9.8%) postprocedure failure. Patient phonatory functions showed significant improvements in shimmer, harmonic-to-noise ratio, phonation time (p < 0.05), grade, roughness and breathiness (p < 0.001). The videolaryngostroboscopic rating showed significant improvements in vocal fold edge linearity, vocal fold vibration amplitude, and mucosal wave excursion (p < 0.001). Improvements observed through long-term follow-up tended to be less dramatic in patients with recurrent VN than those with nonrecurrent VN. FAMSR is an easy, safe, and fast procedure which should be considered as an option in treating VN patients who either require surgery or do not have the time or perseverance to complete a lengthy program of speech therapy.